
This site is intended for US Healthcare Professionals only.
more than a skin disease
Psoriasis (PsO) is a chronic, systemic, immune-mediated disease that affects approximately 125 million people worldwide.1 According to a World Health Organization Report, prevalence of PsO in countries with published data ranged broadly between regions, from the most common prevalence in northern Europe and least common in eastern Asia.2 Prevalence of PsO in countries ranges between 0.09% and 11.4%, while prevalence in the United States is estimated to be approximately 3% in adults.2,3
Plaque-type PsO, psoriasis vulgaris, is the most common form of PsO and typically manifests as well-defined areas of erythematous, scaly plaques on the scalp, trunk and extremities, although any area might be affected.1 While it is often characterized as predominantly a skin disease, PsO can be associated with numerous comorbidities affecting multiple organ systems, underscoring the systemic inflammatory burden of the disease.1,3,4
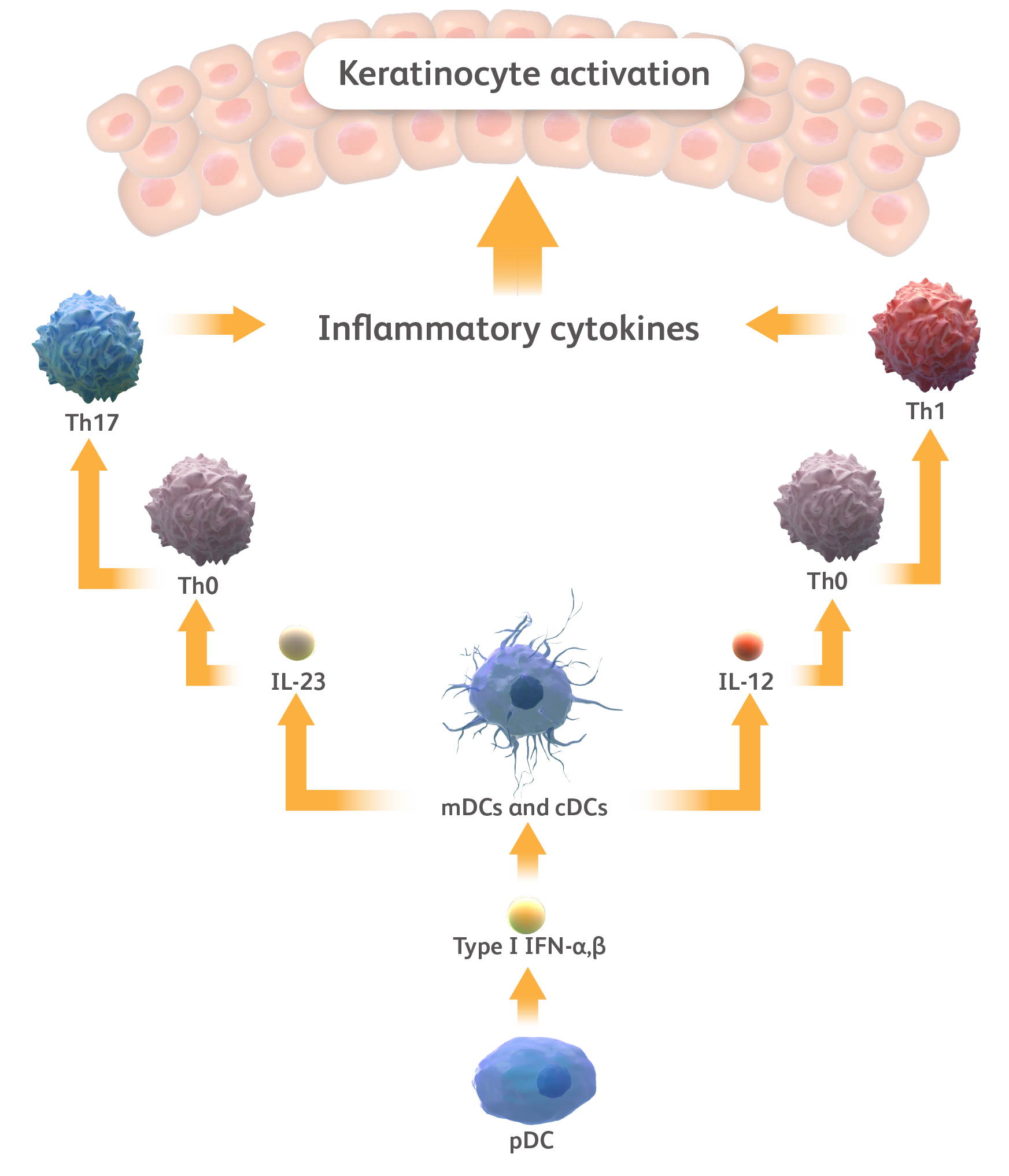
PsO may be initiated via various environmental factors, including trauma, infection, and medications, and certain genetic factors may play a role in certain types of PsO.1 Plasmocytic dendritic cells (DCs) in the skin are activated and release type I interferons (IFNs) that stimulate the activation of myeloid DCs and conventional DCs.5-7 These activated DCs release interleukin (IL)-23 and IL-12, which support and stimulate the differentiation of T helper (Th)17 and Th1 cells, respectively.5,6 These T cells then release additional pro-inflammatory cytokines, most notably the IL-17 family of cytokines, as well as tumor necrosis factor (TNF)-α, interferon (IFN)-γ and IL-22.5,6,8,9 Finally, these cytokines activate keratinocytes, resulting in the formation of psoriatic plaques while also stimulating the release of further cytokines, chemokines, and antimicrobial peptides (AMPs), to propagate the pathogenic cycle.5,6,10
Mediation of selected cytokine signaling 

Please note that this diagram is not exhaustive and does not include all cell types and cytokines that participate in psoriasis pathogenesis. cDC, conventional dendritic cell; IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper.
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2-S6. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Zhang LJ. Front Immunol. 2019;10:1440.
As PsO develops and the inflammatory cycle is reinforced, a chronic, systemic, inflammatory disease emerges, characterized by the circulation of pro-inflammatory cytokines.1,3 The involvement of the IL-17 family of cytokines has been reported in both lesional and non-lesional psoriatic skin, with higher serum levels of key cytokines, such as IL-17A and TNF-α compared to healthy controls.11-13 IL-19 is also highly upregulated in both psoriatic lesions and at the systemic level, reaching expression levels of several thousand times higher in psoriatic skin compared with healthy skin.14 Widespread inflammation produces disease manifestations that can extend to a range of organ systems.1,3 Exploratory positron emission tomography (PET) studies in 6 patients have found that patients with moderate to severe PsO tend to have subclinical inflammation in the liver, joints, and vascular system.15,16
PsO is associated with numerous co-morbidities affecting various organs, including psoriatic arthritis (PsA), cardiovascular disease (CVD), and inflammatory bowel disease (IBD), among others.3,17,18 The etiologies of many of these co-morbidities share common signaling pathways with the inflammatory cytokines involved in skin lesions.3 Examples include:
Mediation of selected cytokine signaling
Please note that this diagram is not exhaustive and does not include all cell types and cytokines that participate in psoriasis pathogenesis. cDC, conventional dendritic cell; IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper.
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2-S6. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Zhang LJ. Front Immunol. 2019;10:1440.
- PsA: Studies have shown that IL-23 signaling and activation of Th17 cells promote enthesitis at tendon insertion sites.17,19 Additionally, IL-23 and TNF-α are established stimulators of synoviocytes and osteoclast differentiation in the synovia both directly and indirectly via Th17 differentiation, resulting in inflammation, bone erosion, and pathologic bone formation.17,19
- CVD: Epidemiological studies found that patients with PsO have an increased prevalence of high-risk plaque in artery walls and increased risk for cardiovascular (CV) events and death.20 TNF-α and other Th1-produced cytokines promote endothelial dysfunction and the movement of T cells to atherosclerotic plaques, while murine models have shown a contribution of IL-17 to atherogenesis.20,21
- IBD: A Danish nationwide prospective cohort study found that patients with PsO have an increased risk of IBD and the risk was highest in patients with severe PsO.18 Genes that encode for proinflammatory cytokines, such as IL12B and IL23R, have been linked to the pathogenesis of both IBD and PsO while increased levels of IL-17 have been reported in IBD patients to drive immune cell recruitment to the gut.22,23,24
The conditions described above are not a comprehensive list, but highlight a selection of common PsO comorbidities.3,4 PsO is an immune-mediated inflammatory disease that can be associated with comorbidities affecting multiple organ systems.1,3
Comorbidities associated with psoriasis

CVD, cardiovascular disease; IBD, inflammatory bowel disease; PsA, psoriatic arthritis; PsO, psoriasis. Elmets CA et al. J Am Acad Dermatol. 2019;80:1073-1113. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Korman NJ. Br J Dermatol. 2020;182:840-848.
Mediation of selected
cytokine signaling
Please note that this diagram is not exhaustive and does not include all cell types and cytokines that participate in psoriasis pathogenesis. cDC, conventional dendritic cell; IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper.
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2-S6. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Zhang LJ. Front Immunol. 2019;10:1440.
Psoriasis (PsO) is a chronic, systemic, immune-mediated disease that affects approximately 125 million people worldwide.1 According to a World Health Organization Report, prevalence of PsO in countries with published data ranged broadly between regions, from the most common prevalence in northern Europe and least common in eastern Asia.2 Prevalence of PsO in countries ranges between 0.09% and 11.4%, while prevalence in the United States is estimated to be approximately 3% in adults.2,3
Plaque-type PsO, psoriasis vulgaris, is the most common form of PsO and typically manifests as well-defined areas of erythematous, scaly plaques on the scalp, trunk and extremities, although any area might be affected.1 While it is often characterized as predominantly a skin disease, PsO can be associated with numerous comorbidities affecting multiple organ systems, underscoring the systemic inflammatory burden of the disease.1,3,4
Mediation of selected
cytokine signaling
Please note that this diagram is not exhaustive and does not include all cell types and cytokines that participate in psoriasis pathogenesis. cDC, conventional dendritic cell; IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper.
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2-S6. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Zhang LJ. Front Immunol. 2019;10:1440.
PsO may be initiated via various environmental factors, including trauma, infection, and medications, and certain genetic factors may play a role in certain types of PsO.1 Plasmocytic dendritic cells (DCs) in the skin are activated and release type I interferons (IFNs) that stimulate the activation of myeloid DCs and conventional DCs.5-7 These activated DCs release interleukin (IL)-23 and IL-12, which support and stimulate the differentiation of T helper (Th)17 and Th1 cells, respectively.5,6 These T cells then release additional pro-inflammatory cytokines, most notably the IL-17 family of cytokines, as well as tumor necrosis factor (TNF)-α, interferon (IFN)-γ and IL-22.5,6,8,9 Finally, these cytokines activate keratinocytes, resulting in the formation of psoriatic plaques while also stimulating the release of further cytokines, chemokines, and antimicrobial peptides (AMPs), to propagate the pathogenic cycle.5,6,10
Mediation of selected
cytokine signaling
Please note that this diagram is not exhaustive and does not include all cell types and cytokines that participate in psoriasis pathogenesis. cDC, conventional dendritic cell; IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper.
Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2-S6. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Zhang LJ. Front Immunol. 2019;10:1440.
As PsO develops and the inflammatory cycle is reinforced, a chronic, systemic, inflammatory disease emerges, characterized by the circulation of pro-inflammatory cytokines.1,3 The involvement of the IL-17 family of cytokines has been reported in both lesional and non-lesional psoriatic skin, with higher serum levels of key cytokines, such as IL-17A and TNF-α compared to healthy controls.11-13 IL-19 is also highly upregulated in both psoriatic lesions and at the systemic level, reaching expression levels of several thousand times higher in psoriatic skin compared with healthy skin.14 Widespread inflammation produces disease manifestations that can extend to a range of organ systems.1,3 Exploratory positron emission tomography (PET) studies in 6 patients have found that patients with moderate to severe PsO tend to have subclinical inflammation in the liver, joints, and vascular system.15,16
PsO is associated with numerous co-morbidities affecting various organs, including psoriatic arthritis (PsA), cardiovascular disease (CVD), and inflammatory bowel disease (IBD), among others.3,17,18 The etiologies of many of these co-morbidities share common signaling pathways with the inflammatory cytokines involved in skin lesions.3
Comorbidities associated
with psoriasis
CVD, cardiovascular disease; IBD, inflammatory bowel disease; PsA, psoriatic arthritis; PsO, psoriasis. Elmets CA et al. J Am Acad Dermatol. 2019;80:1073-1113. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Korman NJ. Br J Dermatol. 2020;182:840-848.
Examples include:
- PsA: Studies have shown that IL-23 signaling and activation of Th17 cells promote enthesitis at tendon insertion sites.17,19 Additionally, IL-23 and TNF-α are established stimulators of synoviocytes and osteoclast differentiation in the synovia both directly and indirectly via Th17 differentiation, resulting in inflammation, bone erosion, and pathologic bone formation.17,19
- CVD: Epidemiological studies found that patients with PsO have an increased prevalence of high-risk plaque in artery walls and increased risk for cardiovascular (CV) events and death.20 TNF-α and other Th1-produced cytokines promote endothelial dysfunction and the movement of T cells to atherosclerotic plaques, while murine models have shown a contribution of IL-17 to atherogenesis.20,21
- IBD: A Danish nationwide prospective cohort study found that patients with PsO have an increased risk of IBD and the risk was highest in patients with severe PsO.18 Genes that encode for proinflammatory cytokines, such as IL12B and IL23R, have been linked to the pathogenesis of both IBD and PsO while increased levels of IL-17 have been reported in IBD patients to drive immune cell recruitment to the gut.22,23,24
Comorbidities associated
with psoriasis
CVD, cardiovascular disease; IBD, inflammatory bowel disease; PsA, psoriatic arthritis; PsO, psoriasis. Elmets CA et al. J Am Acad Dermatol. 2019;80:1073-1113. Greb JE et al. Nat Rev Dis Primers. 2016;2:16082. Korman NJ. Br J Dermatol. 2020;182:840-848.
The conditions described above are not a comprehensive list, but highlight a selection of common PsO comorbidities.3,4 PsO is an immune-mediated inflammatory disease that can be associated with comorbidities affecting multiple organ systems.1,3
References
- Greb JE et al. Nat Rev Dis Primers. 2016;2:16082.
- World Health Organization. Accessed March 24, 2022. https://apps.who.int/iris/handle/10665/204417.
- Korman NJ. Br J Dermatol. 2020;182:840−848.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073−1113.
- Hawkes JE et al. J Immunol. 2018;201:1605−1613.
- Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(5 suppl 93):S2−S6.
- Zhang LJ. Front Immunol. 2019;10:1440.
- Rendon A, Schäkel K. Int J Mol Sci. 2019;20:1475.
- Afonina IS et al. Cell Mol Life Sci. 2021;78:2709−2727.
- Furue M et al. Int J Mol Sci. 2020;21:1275.
- Liu T et al. Front Immunol. 2020;11:594735.
- De Oliveira PSS et al. Mediators Inflamm. 2015;2015:819149.
- Suárez-Fariñas M et al. J Invest Dermatol. 2012;132:2552−2564.
- Witte E et al. J Invest Dermatol. 2014;134:2757−2767.
- Youn SW et al. J Dermatol. 2015;42:559−566.
- Mehta NN, et al. Arch Dermatol. 2011;147:1031−1039.
- Ritchlin CT et al. N Engl J Med. 2017;376:957−970.
- Egeberg A et al. Br J Dermatol. 2016;175:487–492.
- Boutet MA et al. Int J Mol Sci. 2018;19:530.
- Sanda GE et al. Curr Atheroscler Rep. 2017;19:53.
- Armstrong AW et al. Exp Dermatol. 2011;20:544−549.
- Fujino S et al. Gut. 2003;52:65–70.
- Fu Y et al. JAMA Dermatol. 2018;154:1417–1423.
- de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13–27.