
This site is intended for US Healthcare Professionals only.
more than a skin disease
Cardiovascular Disease
Patients suffering from psoriasis (PsO) are at a higher risk of developing cardiovascular disease (CVD) compared with the general population.1−3,6 PsO is an independent risk factor for myocardial infarction (MI), stroke, vascular inflammation, and for the prevalence of coronary atherosclerotic plaques and severe coronary calcification.1−7 Even mild disease confers a significantly increased risk of stroke, MI and coronary revascularization in patients with PsO.4,8 In the US, mild and severe PsO may be associated with up to 11,500 excess major adverse cardiovascular events each year.4 In addition to severe skin disease, development of PsO at a young age and the presence of psoriatic arthritis (PsA) are additional risk factors for CVD in patients with PsO.5,9,10
Cardiovascular Disease
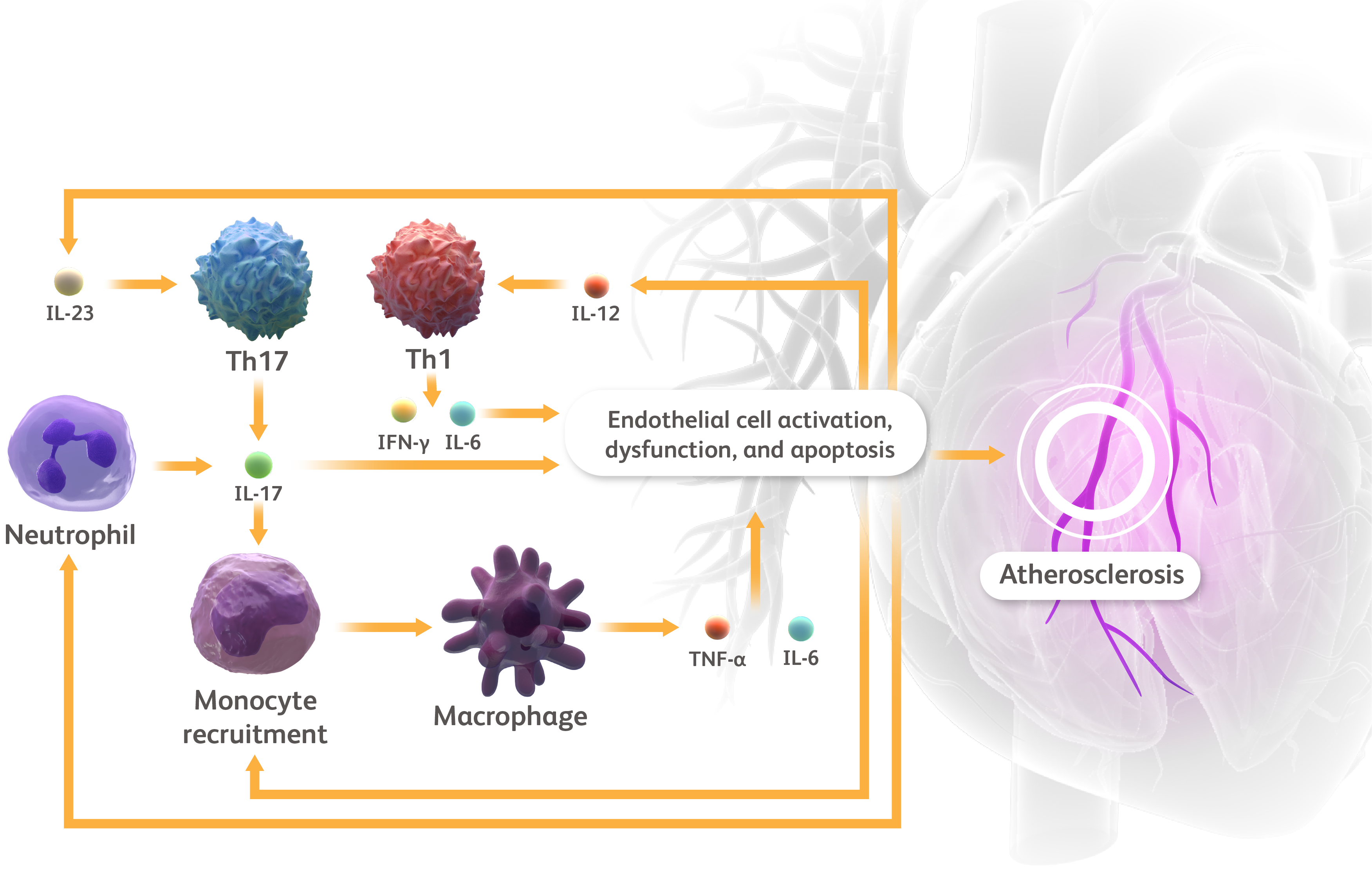
IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
Cardiovascular Disease
While it is unknown if the mechanisms associated with CVD are shared in patients with and without PsO, a complex interplay between inflammation and immune response is involved in the pathophysiology of the two diseases.11-14 For instance, interleukin (IL)-17 signaling, resulting partially from upstream IL-23 signaling, stimulates skin plaque formation in PsO and is also implicated in the development of atherosclerosis.13,16 Likewise, interferon-gamma (IFN y) and tumor necrosis factor (TNF-α), cytokines produced by Th1 cells in response to IL-12, act on keratinocytes to drive an inflammatory cascade in psoriasis and may also be involved in atherosclerotic plaque formation.13,17-19 In resting blood vessels, IL-17 and neutrophils can activate endothelial cells, which in turn release cytokines and chemokines that potentiate inflammation.16 Inflammatory cytokines such as IL-6 and TNF-α also act downstream of IL-17 and may promote cardiovascular co-morbidity.14,20-22 In essence, mechanistic similarities between PsO and atherosclerosis support a role for inflammation shared among the disease states.11,13,16
Cardiovascular Disease
IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
Cardiovascular Disease
According to the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that dermatologists inform patients with PsO of their increased risk of CVD and need for appropriate screening by their primary care provider or cardiologist.11 This screening may include height, weight, body mass index, abdominal circumference, blood glucose, glycosylated hemoglobin, and fasting lipid levels.11 If needed, recommendations for lifestyle modification (eg, dietary changes, exercise regimens, and advice on smoking cessation) and/or a referral for specialist care might also be warranted.11
Cardiovascular Disease
IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
Cardiovascular Disease

IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
Patients suffering from psoriasis (PsO) are at a higher risk of developing cardiovascular disease (CVD) compared with the general population.1−3,6 PsO is an independent risk factor for myocardial infarction (MI), stroke, vascular inflammation, and for the prevalence of coronary atherosclerotic plaques and severe coronary calcification.1−7 Even mild disease confers a significantly increased risk of stroke, MI and coronary revascularization in patients with PsO.4,8 In the US, mild and severe PsO may be associated with up to 11,500 excess major adverse cardiovascular events each year.4 In addition to severe skin disease, development of PsO at a young age and the presence of psoriatic arthritis (PsA) are additional risk factors for CVD in patients with PsO.5,9,10
Cardiovascular Disease
IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
While it is unknown if the mechanisms associated with CVD are shared in patients with and without PsO, a complex interplay between inflammation and immune response is involved in the pathophysiology of the two diseases.11-14 For instance, interleukin (IL)-17 signaling, resulting partially from upstream IL-23 signaling, stimulates skin plaque formation in PsO and is also implicated in the development of atherosclerosis.13,16 Likewise, interferon-gamma (IFN y) and tumor necrosis factor (TNF-α), cytokines produced by Th1 cells in response to IL-12, act on keratinocytes to drive an inflammatory cascade in psoriasis and may also be involved in atherosclerotic plaque formation.13,17-19 In resting blood vessels, IL-17 and neutrophils can activate endothelial cells, which in turn release cytokines and chemokines that potentiate inflammation.16 Inflammatory cytokines such as IL-6 and TNF-α also act downstream of IL-17 and may promote cardiovascular co-morbidity.14,20-22 In essence, mechanistic similarities between PsO and atherosclerosis support a role for inflammation shared among the disease states.11,13,16
Cardiovascular Disease
IFN, interferon; IL, interleukin; Th, T helper; TNF-α, tumor necrosis factor-alpha.
Eid RE et al. Circulation. 2009;119:1424-1432. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-2668. Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345-352. Sanda GE et al. Curr Atheroscler Rep. 2017;19:53. Von Stebut E et al. Front Immunol. 2020;10:3096. Wang Y et al. Front Immunol. 2022;13:835671. Zhang S et al. PLoS ONE. 2012;7(7): e40641.
According to the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that dermatologists inform patients with PsO of their increased risk of CVD and need for appropriate screening by their primary care provider or cardiologist.11 This screening may include height, weight, body mass index, abdominal circumference, blood glucose, glycosylated hemoglobin, and fasting lipid levels.11 If needed, recommendations for lifestyle modification (eg, dietary changes, exercise regimens, and advice on smoking cessation) and/or a referral for specialist care might also be warranted.11
References
- Samarasekera EJ et al. J Invest Dermatol. 2013;133:2340−2346.
- Dey AK et al. JAMA Cardiol. 2017;2(9):1013–1018.
- Lerman JB et al. Circulation. 2017;136:263–276.
- Armstrong EJ et al. J Am Heart Assoc. 2013;4:2:e000062.
- Armstrong AW, Read C. JAMA. 2020;323:1945–1960.
- Armstrong AW et al. Am J Cardiol. 2012;109:976–980.
- Tinggaard AB et al. J Intern Med. 2021;290(3):693–703.
- Ahlehoff O et al. J Intern Med. 2011;270:147–157.
- Gelfand JM et al. J Am Acad Dermatol. 2006;55:829–835.
- Skornicki M et al. Adv Ther. 2021;38:2458–2471.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073–1113.
- Ghazizadeh R et al. Int J Med Sci. 2010;7:284–289.
- Lockshin B et al. J Am Acad Dermatol. 2018;79(2):345–352.
- Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658–68.
- Zhang S et al. PLoS ONE. 2012;7(7): e40641.
- Sanda GE et al. Curr Atheroscler Rep. 2017;19:53.
- Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33:S2−S6.
- Wang Y et al. Front Immunol. 2022;13:835671.
- Mehta NN et al. Sci Rep. 2017;7:13831.
- Von Steubt E et al. Front Immunol. 2020;10:3096.
- Garshick MS et al. Arterioscler Thromb Vasc Biol. 2019;39:787–798
- Verma D et al. J Invest Dematol. 2021;141:586–595.