
This site is intended for US Healthcare Professionals only.
more than a skin disease
Psoriatic Arthritis
Psoriatic arthritis (PsA) is a systemic inflammatory disorder and common comorbidity of psoriasis (PsO) characterized by stiffness, pain, swelling of the joints, sites of tendon or ligament insertion (entheses), and/or the potential for axial (spinal) disease that can progress to debilitating joint destruction.1–3 PsA affects approximately one-third of patients with PsO and typically manifests 7-12 years after the onset of PsO.1,2 In the vast majority (75%-80%) of patients with PsA, skin disease precedes joint disease.1 While 91% of patients with PsA are reported to have peripheral joint disease, patients can also show symptoms such as axial involvement (estimated 25%-70% of patients with PsA), enthesitis (pooled estimate of 30% of patients with PsA, with a range of 6.3%-72%), dactylitis (inflammation of an entire digit/“sausage digit”; pooled estimate of 25%, with a range of 1.5%-59%), and psoriatic nail disease (pooled estimate of 60%, with a range of 26%-92%).2-6 Worse outcomes, including joint damage and loss of function, have been reported with a delay in diagnosis of PsA of as little as 6 months.7
Psoriatic Arthritis
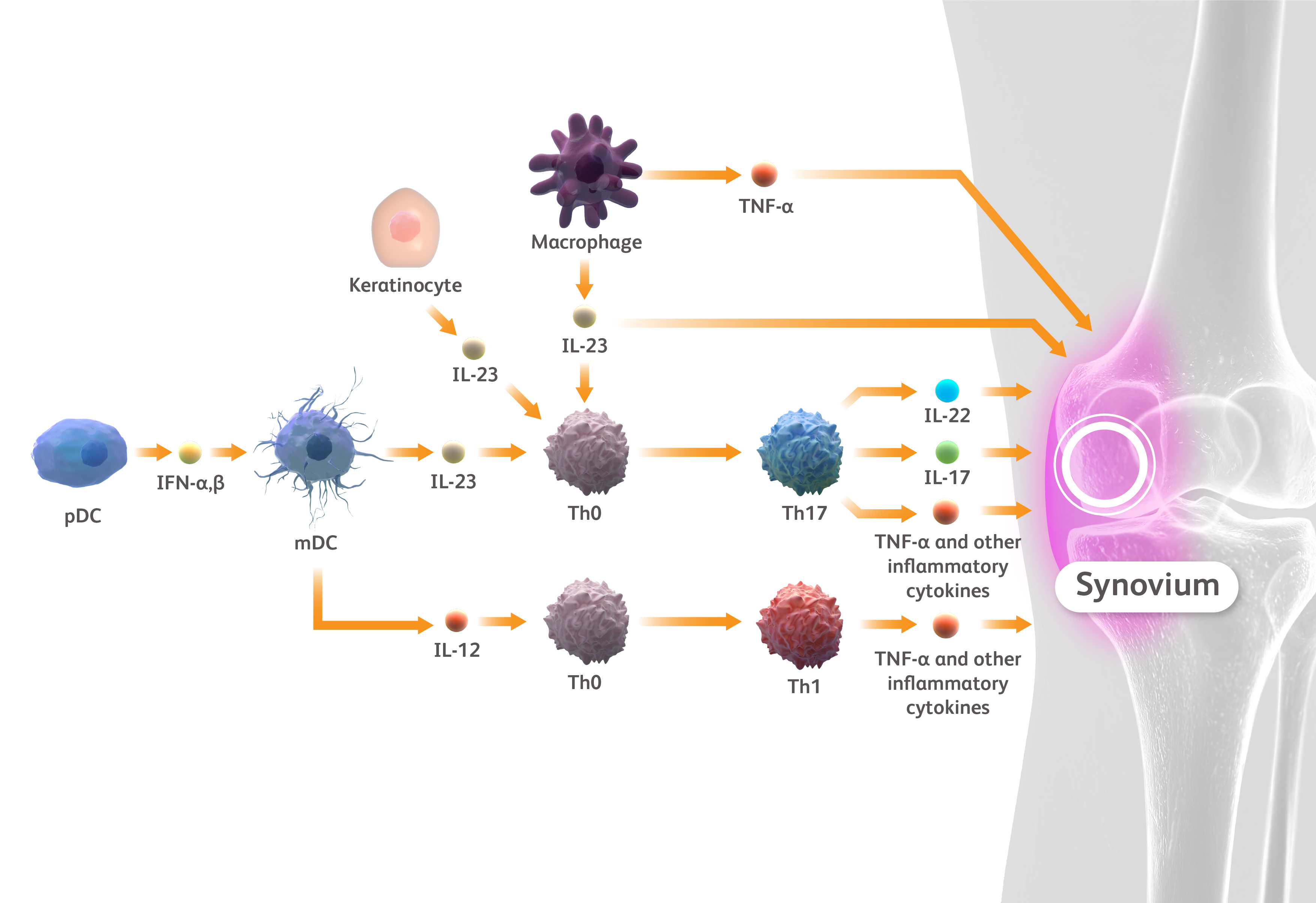
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
Psoriatic Arthritis
The development of PsA is currently understood to be caused by a combination of immune, genetic, and environmental factors, and the risk of developing PsA increases steadily with the severity and duration of PsO.1,8-11 The two conditions share certain common pathogenic mechanisms, including the overactivation of proinflammatory cytokines such as interleukin (IL)-23.1 Additionally, increased numbers of circulating T helper (Th)22 and Th17 cells have been identified in both PsO and PsA, and the IL-23/IL-17 axis has been shown to play a critical role in the mechanism of both diseases.12–16 Dendritic cells activated by different stimuli secrete IL-23 and IL-12, which further activate the immune system, leading to the production of inflammatory cytokines such as TNF-α, IL-22, IFN-γ, and IL-17.12 In PsO, IL-17 activates keratinocytes, stimulating the formation of psoriatic plaques.13 In PsA, the release of IL-22 at the tendon insertion site contributes to the differentiation of mesenchymal cells into osteoblasts, causing pathologic bone formation that can lead to bony ankylosis.14 At the same time, IL-17 contributes to the differentiation of osteoclasts, which can induce synovitis and bone resorption in the joint, while IL-23 also causes direct inflammation in the synovium.8,13,14
Psoriatic Arthritis
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
Psoriatic Arthritis
Because patients may experience irreversible joint damage when untreated, a proactive approach to PsA screening is imperative.9 PsA remains at present a clinical diagnosis.17 According to one guideline, the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that dermatologists screen patients with PsO for PsA at each visit by using a combination of screening tools, clinical assessment, and potentially musculoskeletal imaging. Validated screening tools, including the Psoriasis Epidemiology Screening Tool and others, are sensitive to the detection of potential disease and have a low burden on providers and staff.9,18–21 Increased awareness of this complex comorbidity of PsO is important for effective patient monitoring, treatment, and comanagement—where appropriate—with rheumatologists.9,18
Psoriatic Arthritis
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
Psoriatic Arthritis
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
Psoriatic arthritis (PsA) is a systemic inflammatory disorder and common comorbidity of psoriasis (PsO) characterized by stiffness, pain, swelling of the joints, sites of tendon or ligament insertion (entheses), and/or the potential for axial (spinal) disease that can progress to debilitating joint destruction.1–3 PsA affects approximately one-third of patients with PsO and typically manifests 7-12 years after the onset of PsO.1,2 In the vast majority (75%-80%) of patients with PsA, skin disease precedes joint disease.1 While 91% of patients with PsA are reported to have peripheral joint disease, patients can also show symptoms such as axial involvement (estimated 25%-70% of patients with PsA), enthesitis (pooled estimate of 30% of patients with PsA, with a range of 6.3%-72%), dactylitis (inflammation of an entire digit/“sausage digit”; pooled estimate of 25%, with a range of 1.5%-59%), and psoriatic nail disease (pooled estimate of 60%, with a range of 26%-92%).2-6 Worse outcomes, including joint damage and loss of function, have been reported with a delay in diagnosis of PsA of as little as 6 months.7
Psoriatic Arthritis
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
The development of PsA is currently understood to be caused by a combination of immune, genetic, and environmental factors, and the risk of developing PsA increases steadily with the severity and duration of PsO.1,8-11 The two conditions share certain common pathogenic mechanisms, including the overactivation of proinflammatory cytokines such as interleukin (IL)-23.1 Additionally, increased numbers of circulating T helper (Th)22 and Th17 cells have been identified in both PsO and PsA, and the IL-23/IL-17 axis has been shown to play a critical role in the mechanism of both diseases.12–16 Dendritic cells activated by different stimuli secrete IL-23 and IL-12, which further activate the immune system, leading to the production of inflammatory cytokines such as TNF-α, IL-22, IFN-γ, and IL-17.12 In PsO, IL-17 activates keratinocytes, stimulating the formation of psoriatic plaques.13 In PsA, the release of IL-22 at the tendon insertion site contributes to the differentiation of mesenchymal cells into osteoblasts, causing pathologic bone formation that can lead to bony ankylosis.14 At the same time, IL-17 contributes to the differentiation of osteoclasts, which can induce synovitis and bone resorption in the joint, while IL-23 also causes direct inflammation in the synovium.8,13,14
Psoriatic Arthritis
IFN, interferon; IL, interleukin; mDC, myeloid dendritic cell; pDC, plasmacytoid dendritic cell; Th, T helper; TNF, tumor necrosis factor.
Boutet MA et al. Int J Mol Sci. 2018;19:530. Ritchlin CT et al. N Engl J Med. 2017;376:957-970. Jang D et al. Int J Mol Sci. 2021;22:2719
Because patients may experience irreversible joint damage when untreated, a proactive approach to PsA screening is imperative.9 PsA remains at present a clinical diagnosis.17 According to one guideline, the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that dermatologists screen patients with PsO for PsA at each visit by using a combination of screening tools, clinical assessment, and potentially musculoskeletal imaging. Validated screening tools, including the Psoriasis Epidemiology Screening Tool and others, are sensitive to the detection of potential disease and have a low burden on providers and staff.9,18–21 Increased awareness of this complex comorbidity of PsO is important for effective patient monitoring, treatment, and comanagement—where appropriate—with rheumatologists.9,18
References
- Mease PJ, Armstrong AW. Drugs. 2014;74:423–441.
- Armstrong AW, Read C. JAMA. 2020;323:1945–1960.
- Gottlieb AB, Merola JF. J Am Acad Dermatol. 2021;84:92–101.
- López-Medina C et al. RMD Open. 2021;7:e001450.
- Poddubnyy D et al. Semin Arthritis Rheum. 2021;51:880–887.
- Pittam B et al. Rheumatology (Oxford). 2020;59:2199–2206.
- Haroon M et al. Ann Rheum Dis. 2015;74:1045–1050.
- Carvahlo AL, Hedrich CM. Front Mol Biosci. 2021;8:662047.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073–1113.
- Alinaghi F et al. J Am Acad Dermatol. 2019;80:251–265.e19.
- Merola JF et al. J Am Acad Dermatol. 2022;86:748–757.
- Veale DJ, Fearon U. Lancet. 2018;391:2273–2284.
- Boutet MA et al. Int J Mol Sci. 2018;19:530.
- Ritchlin CT et al. N Engl J Med. 2017;376:957–970.
- Georgescu SR et al. Int J Mol Sci. 2019;20:739.
- Benham H et al. Arthritis Res Ther. 2013;15(5):R136. doi: 10.1186/ar4317.
- Leung YY et al. Front Med (Lausanne). 2018;5:246.
- Gottlieb AB et al. Dermatol Ther (Heidelb). 2021;11:1199–1216.
- Tom BDM et al. J Rheumatol. 2015;42:841–846.
- Husni ME et al. J Am Acad Dermatol. 2007;57:581–587.
- Helliwell PS. J Rheumatol. 2011;38:551–552.