
This site is intended for US Healthcare Professionals only.
more than a skin disease
Renal Disease
Chronic kidney disease (CKD) involves a gradual loss of kidney function resulting in progressive loss of the ability to excrete phosphorus.1 A major health problem, CKD affects 10% of adults and >20% of people over 60 years of age.1 The association between impaired renal function and onset of cardiovascular disease (CVD) is especially troubling, with the risk of CVD in patients with end-stage renal disease being 20−30 times that of the general population.1,2 While many co-morbidities of psoriasis (PsO) can negatively affect the kidneys, moderate to severe PsO is an independent risk factor for CKD, even after adjustment for confounders.3−5 The odds of CKD increase with PsO severity, and a greater prevalence of microalbuminuria, a sign of sub-clinical glomerular dysfunction, has been reported in patients with PsO.3,6−8
Renal Disease
Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
Renal Disease
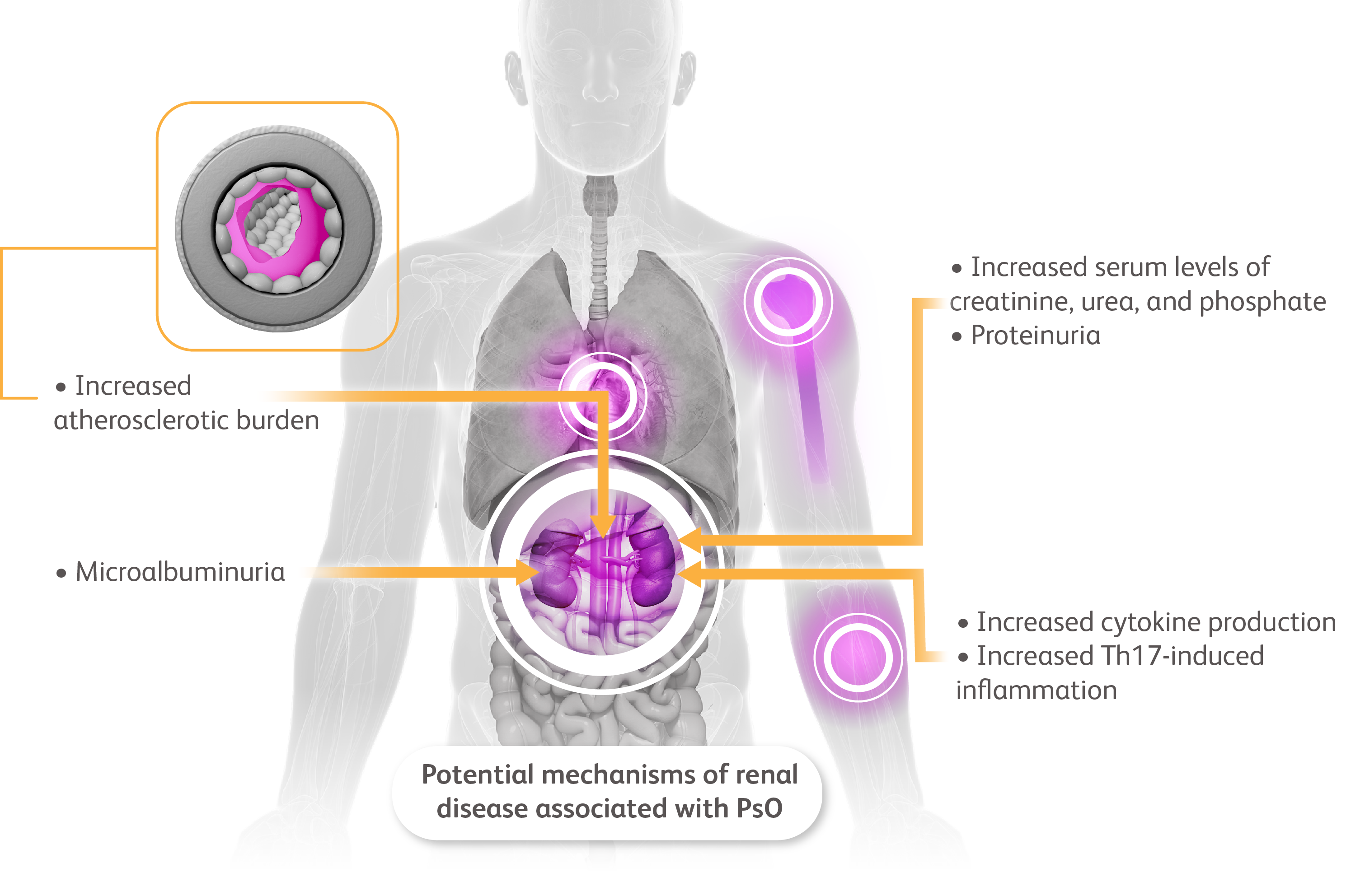
Although the exact mechanisms of this association are not completely elucidated, renal disease may stem from inflammatory changes within the kidney microvasculature.9,10 The development of chronic renal failure in patients with PsO may be connected to a chronic inflammatory state driven by increased cytokine production.11 Patients with PsO are also known to have a higher atherosclerotic burden than the general population because of chronic damage to endothelial cells derived from prolonged inflammation.4,11 Hence, accelerated atherosclerosis could be a link among PsO, CKD, and CVD.4 Mechanistically, the direct induction of inflammation by T helper (Th)1 and Th17 lymphocytes, which are involved in the pathogenesis of PsO, has been shown to also induce direct inflammation in the kidneys by mediating tubular epithelial cells, mesangial cells, and macrophages.4,12−15
Renal Disease
Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
Renal Disease
It is important that dermatologists remain aware of the independent association of CKD and PsO.5 Because the association is strongest in patients with severe psoriasis, testing may be considered more frequently in such patients.5 According to one guideline, the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that in addition to blood urea nitrogen and creatinine, urinary microalbumin should be assessed to detect occult renal disease.5 When managing patients with PsO and comorbid CKD, dermatologists should carefully consider duration, dosing and drug-interactions of potentially nephrotoxic treatments.3,5,16
Patients with evidence of CKD should be referred to their primary care provider or a nephrologist for further assessment and management.5
Renal Disease
Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
Renal Disease
Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
Chronic kidney disease (CKD) involves a gradual loss of kidney function resulting in progressive loss of the ability to excrete phosphorus.1 A major health problem, CKD affects 10% of adults and >20% of people over 60 years of age.1 The association between impaired renal function and onset of cardiovascular disease (CVD) is especially troubling, with the risk of CVD in patients with end-stage renal disease being 20−30 times that of the general population.1,2 While many co-morbidities of psoriasis (PsO) can negatively affect the kidneys, moderate to severe PsO is an independent risk factor for CKD, even after adjustment for confounders.3−5 The odds of CKD increase with PsO severity, and a greater prevalence of microalbuminuria, a sign of sub-clinical glomerular dysfunction, has been reported in patients with PsO.3,6−8
Renal Disease

Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
Although the exact mechanisms of this association are not completely elucidated, renal disease may stem from inflammatory changes within the kidney microvasculature.9,10 The development of chronic renal failure in patients with PsO may be connected to a chronic inflammatory state driven by increased cytokine production.11 Patients with PsO are also known to have a higher atherosclerotic burden than the general population because of chronic damage to endothelial cells derived from prolonged inflammation.4,11 Hence, accelerated atherosclerosis could be a link among PsO, CKD, and CVD.4 Mechanistically, the direct induction of inflammation by T helper (Th)1 and Th17 lymphocytes, which are involved in the pathogenesis of PsO, has been shown to also induce direct inflammation in the kidneys by mediating tubular epithelial cells, mesangial cells, and macrophages.4,12−15
Renal Disease
Th, T helper. Chiu H-Y et al. Br J Dermatol. 2015;173:146-154. González-Parra E et al. Actas Dermosifiliogr. 2016;107:823-829.
Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397. Szepietowski JC et al. J Eur Acad Dermatol Venereol.
2000;14:513-514. Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277-1283.
It is important that dermatologists remain aware of the independent association of CKD and PsO.5 Because the association is strongest in patients with severe psoriasis, testing may be considered more frequently in such patients.5 According to one guideline, the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that in addition to blood urea nitrogen and creatinine, urinary microalbumin should be assessed to detect occult renal disease.5 When managing patients with PsO and comorbid CKD, dermatologists should carefully consider duration, dosing and drug-interactions of potentially nephrotoxic treatments.3,5,16
Patients with evidence of CKD should be referred to their primary care provider or a nephrologist for further assessment and management.5
References
- González-Parra E et al. Actas Dermosifiliogr. 2016;107:823−829.
- Berl T, Henrich W. Clin J Am Soc Nephrol. 2006;1:8−18.
- Takeshita J et al. J Am Acad Dermatol. 2017;76:377−390.
- Ungprasert P, Raksasuk S. Int Urol Nephrol. 2018;50:1277−1283.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073−1113.
- Tehranchinia Z et al. ScientificWorldJournal. 2018;2018:5301631.
- Szepietowski JC et al. J Eur Acad Dermatol Venereol. 2000;14:513−514.
- Cecchi R et al. Dermatology. 1992;185:93−95.
- Bilal J et al. Am J Med. 2018;131:1146−1154.
- Chi CC et al. J Dermatol Sci. 2015;78:232−238.
- Visconti L et al. Clin Rheumatol. 2016;35:297−302.
- Shahwan KT, Kimball AB. Med Clin North Am. 2015;99:1227−1242.
- Ogawa E et al. J Dermatol. 2018;45:264−272.
- Turner J-E et al. Kidney Int. 2010;77:1070−1075.
- Kitching AR, Holdsworth SR. J Am Soc Nephrol. 2011;22:235−238.
- Chiu H-Y et al. Br J Dermatol. 2015;173:146−154.