
This site is intended for US Healthcare Professionals only.
more than a skin disease
Non-Alcoholic Fatty Liver Disease
Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disorder worldwide, affecting nearly 30% of the population in developed countries.1–4 NAFLD encompasses a spectrum of disorders ranging from steatosis, in which fat builds up in the liver but liver cells are not yet damaged, to non-alcoholic steatohepatitis (NASH), which is characterized by chronic liver inflammation and is the leading cause of fibrosis, cirrhosis, and hepatocellular carcinoma.1–3,5–7 Once cirrhosis develops, complications often arise, leading to an estimated 5-year mortality rate of about 25%.8,9
Patients with psoriasis (PsO) have a 1.5–3-fold higher prevalence of NAFLD, a higher rate of severe disease, and a worse prognosis than non-psoriatic controls.8 The risk of developing NAFLD increases with PsO severity.10–14 Notably, PsO is associated with NAFLD even after adjusting for metabolic syndrome traits and other potential confounding factors.10–14
Non-Alcoholic Fatty Liver Disease
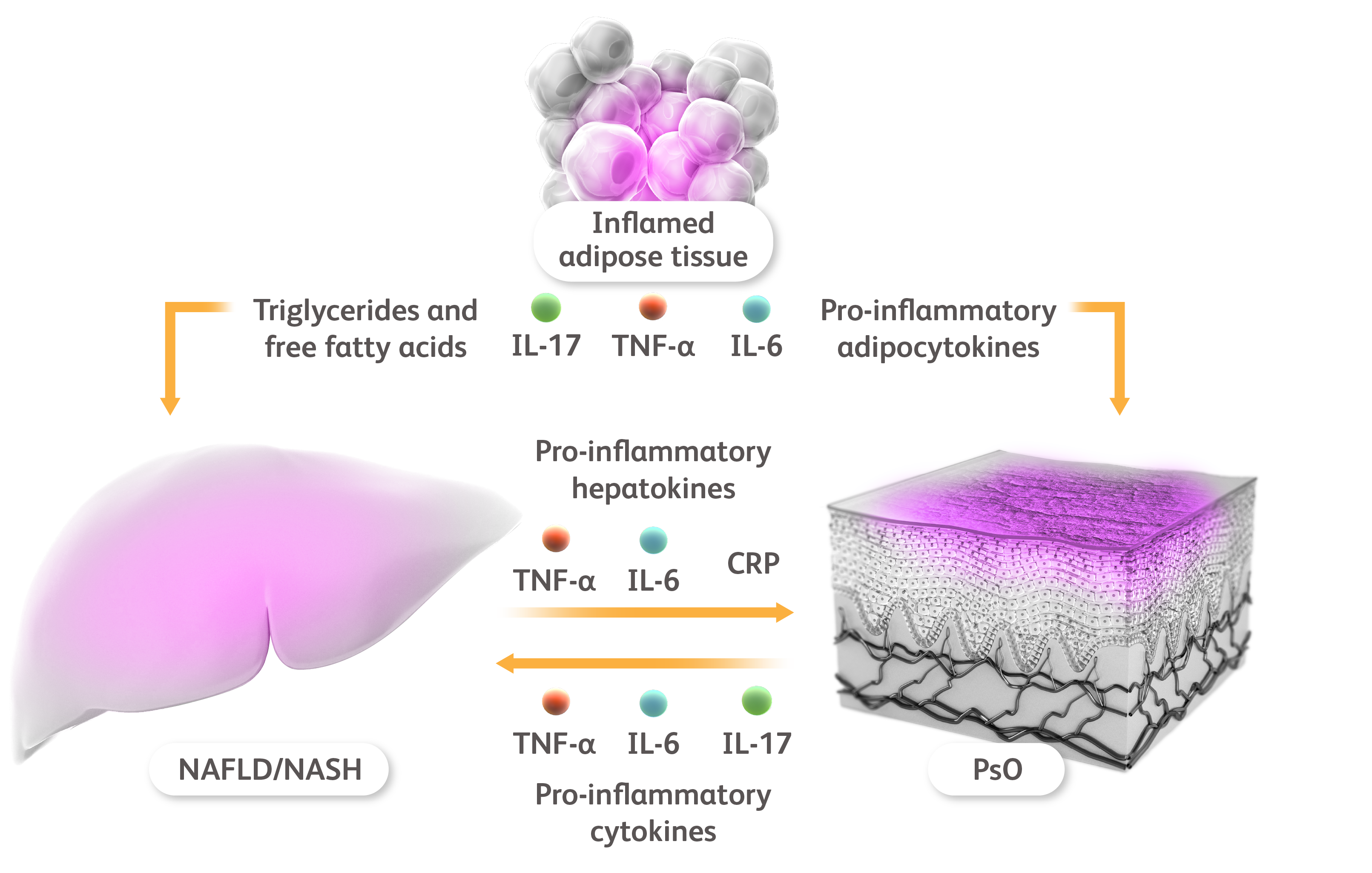
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Non-Alcoholic Fatty Liver Disease
Chronic ongoing low-grade inflammation is a common feature of both PsO and NAFLD, which seem to be connected by a shared T helper (Th)17 inflammatory axis, and by the action of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin (IL)-6, and IL-17.2,12,15 The role of IL-17 is especially critical to the pathogenesis of both conditions. In PsO, IL-17 promotes inflammation via activation of keratinocytes, which ultimately leads to the development of psoriatic plaques.16 In NAFLD, IL-17 stimulation leads to increased release of free fatty acids by white adipose tissue, increased hepatocyte lipid uptake, and hepatocyte-driven cytokine production, rendering hepatocytes particularly susceptible to damage.17
Early identification of the presence of NAFLD in patients with chronic PsO is important to help prevent liver damage.2,4 Increased dermatologist awareness of the increased prevalence of NAFLD in patients with PsO is especially relevant for patients with metabolic syndrome and/or psoriatic arthritis (PsA), who are particularly at risk.4 Patients with NAFLD may be referred to a hepatologist for further evaluation and follow-up.2,8
Non-Alcoholic Fatty Liver Disease
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Non-Alcoholic Fatty Liver Disease
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Non-alcoholic fatty liver disease (NAFLD) is the most common chronic liver disorder worldwide, affecting nearly 30% of the population in developed countries.1–4 NAFLD encompasses a spectrum of disorders ranging from steatosis, in which fat builds up in the liver but liver cells are not yet damaged, to non-alcoholic steatohepatitis (NASH), which is characterized by chronic liver inflammation and is the leading cause of fibrosis, cirrhosis, and hepatocellular carcinoma.1–3,5–7 Once cirrhosis develops, complications often arise, leading to an estimated 5-year mortality rate of about 25%.8,9
Non-Alcoholic Fatty Liver Disease
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Patients with psoriasis (PsO) have a 1.5–3-fold higher prevalence of NAFLD, a higher rate of severe disease, and a worse prognosis than non-psoriatic controls.8 The risk of developing NAFLD increases with PsO severity.10–14 Notably, PsO is associated with NAFLD even after adjusting for metabolic syndrome traits and other potential confounding factors.10–14
Non-Alcoholic Fatty Liver Disease
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Chronic ongoing low-grade inflammation is a common feature of both PsO and NAFLD, which seem to be connected by a shared T helper (Th)17 inflammatory axis, and by the action of pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin (IL)-6, and IL-17.2,12,15 The role of IL-17 is especially critical to the pathogenesis of both conditions. In PsO, IL-17 promotes inflammation via activation of keratinocytes, which ultimately leads to the development of psoriatic plaques.16 In NAFLD, IL-17 stimulation leads to increased release of free fatty acids by white adipose tissue, increased hepatocyte lipid uptake, and hepatocyte-driven cytokine production, rendering hepatocytes particularly susceptible to damage.17
Non-Alcoholic Fatty Liver Disease
CRP, C-reactive protein; IL, interleukin; NAFLD, non-alcoholic fatty liver disease; NASH, non-alcoholic steatohepatitis; PsO, psoriasis; TNF-α, tumor necrosis factor α.
Giles DA et al. Curr Drug Targets. 2015;16:1315-1323. Mantovani A et al. Int J Mol Sci. 2016;17:217.
Early identification of the presence of NAFLD in patients with chronic PsO is important to help prevent liver damage.2,4 Increased dermatologist awareness of the increased prevalence of NAFLD in patients with PsO is especially relevant for patients with metabolic syndrome and/or psoriatic arthritis (PsA), who are particularly at risk.4 Patients with NAFLD may be referred to a hepatologist for further evaluation and follow-up.2,8
References
- Tula E et al. Australas J Dermatol. 2017;58:194–199.
- Mantovani A et al. Int J Mol Sci. 2016;17:217.
- Anstee QM et al. Nat Rev Gastroenterol Hepatol. 2013;10:330–344.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073–1113.
- Wenk KS et al. J Eur Acad Dermatol Venereol. 2011;25:383–391.
- Farrell GC et al. J Gastroenterol Hepatol. 2007;22:775–777.
- Angelico F et al. J Gastroenterol Hepatol. 2003;18:588–594.
- Carrascosa JM et al. Actas Dermosifiliogr. 2017;108:506–514.
- Yatsuji S et al. J Gastroenterol Hepatol. 2009;24:248–254.
- Busca Arenzana C et al. Cells. 2021;10:1099.
- Ganzetti G et al. World J Cardiol. 2016;8:120–131.
- Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397.
- Ogdie A. J Invest Dermatol. 2018;138:760–767.
- Candia R et al. J Eur Acad Dermatol Venereol. 2015;29:656–662.
- Heitmann J et al. J Dtsch Dermatol Ges. 2021;19:517–528.
- Afonina IS et al. Cell Mol Life Sci. 2021;78:2709–2727.
- Giles DA et al. Curr Drug Targets. 2015;16:1315–1323.