
This site is intended for US Healthcare Professionals only.
more than a skin disease
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) is a chronic relapsing inflammatory disease of the gastrointestinal tract that can also manifest as a comorbidity of psoriasis (PsO).1 Patients with PsO are estimated to have a 1.71-2.53× higher risk of IBD, depending on the type of IBD.1 Its two most common forms are Crohn’s disease (CD), in which the infiltration of immune cells into the mucosal barrier causes inflammation, resulting in the destruction of the intestinal wall layers along the digestive tract,1-3 and ulcerative colitis (UC), in which the same type of inflammation is primarily localized to the colon and rectum.1,2,4 Patients with IBD often experience recurrent loss of appetite, vomiting, diarrhea, abdominal pain, rectal bleeding, and body weight loss, and they typically require long-term management.1
Inflammatory Bowel Disease
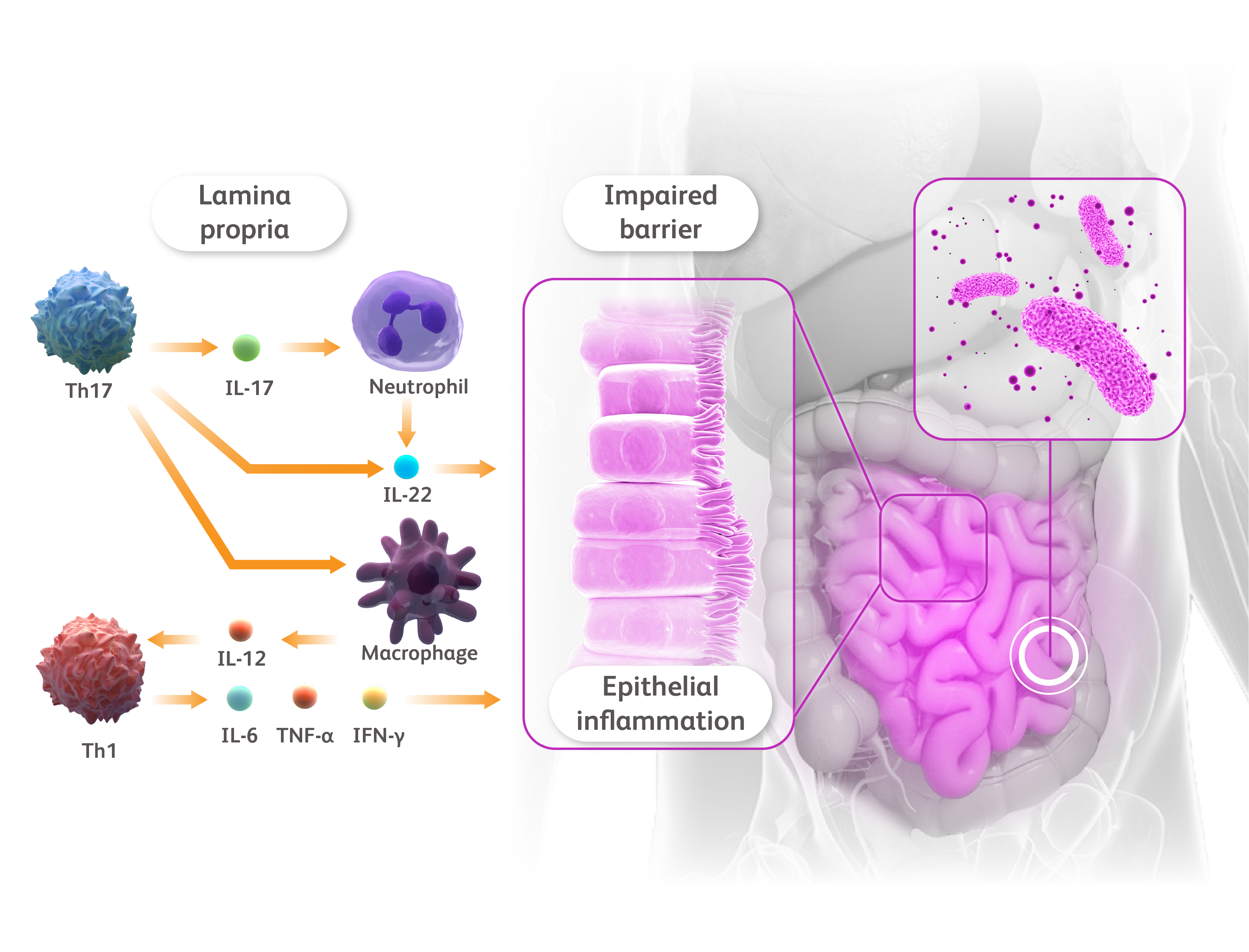
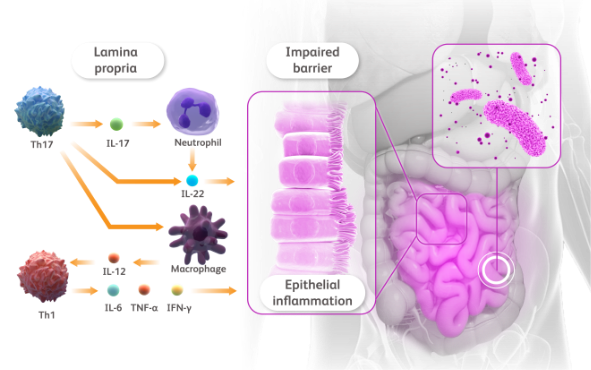
IFN-γ, interferon γ; IL, interleukin; Th, T helper; TNF, tumor necrosis factor.
de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13-27. Salas A et al. Nat Rev Gastroenterol Hepatol. 2020;17:323-337.
Inflammatory Bowel Disease
IBD affects about 0.5% of the general population, but CD and UC have been reported to be 2-4× and 1.6-1.9× as frequent in patients with PsO, respectively.4-7 This known association appears to be rooted in a common dysregulation of the immune response in genetically susceptible individuals; among others, variants in several genes encoding for proinflammatory cytokine signals (eg, interleukin [IL]-12 or the IL-23 receptor) are correlated with both PsO and IBD.1,2,5–9 Notably, IBD is characterized by increased levels of several inflammatory cytokines, including IL-2 and interferon-gamma (IFN-γ) in CD, IL-5 in UC, and IL-17, IL-10, IL-1β, IL-6, and tumor necrosis factor (TNF) in both conditions.10,11 IL-17, IL-6, TNF-α, and IFN-γ are some of the key cytokines also involved in PsO pathogenesis.1,12,13 In the skin epithelium, IL-17 overexpression can trigger an inflammatory cycle, resulting in the formation of psoriatic plaques,13,14 whereas in the lamina propria of the gut, IL-17 supports neutrophil recruitment to promote inflammation and IL-22 mediated epithelial proliferation.10 This immune activation, acting alongside the release of further proinflammatory cytokines secreted by T-helper 1 cells, such as IL-6, TNF, and IFN-γ, inflames the epithelial cells that line the gut and ultimately damages them.10,15 This damage leads to barrier dysfunction, which allows the translocation of microbes into the bowel wall, attracting immune cells and amplifying inflammation.16,17
Inflammatory Bowel Disease
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Inflammatory Bowel Disease
Because of the complex interplay between PsO and IBD, it is important for patients to be informed of their increased risk of developing this condition.4 Monitoring signs and symptoms of digestive tract disease in patients with PsO is especially important, as it would allow dermatologists to promptly refer patients in need for further evaluation and specialist care.4
Inflammatory Bowel Disease
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Inflammatory Bowel Disease
IFN-γ, interferon γ; IL, interleukin; Th, T helper; TNF, tumor necrosis factor.
de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13-27. Salas A et al. Nat Rev Gastroenterol Hepatol. 2020;17:323-337.
Inflammatory bowel disease (IBD) is a chronic relapsing inflammatory disease of the gastrointestinal tract that can also manifest as a comorbidity of psoriasis (PsO).1 Patients with PsO are estimated to have a 1.71-2.53× higher risk of IBD, depending on the type of IBD.1 Its two most common forms are Crohn’s disease (CD), in which the infiltration of immune cells into the mucosal barrier causes inflammation, resulting in the destruction of the intestinal wall layers along the digestive tract,1-3 and ulcerative colitis (UC), in which the same type of inflammation is primarily localized to the colon and rectum.1,2,4 Patients with IBD often experience recurrent loss of appetite, vomiting, diarrhea, abdominal pain, rectal bleeding, and body weight loss, and they typically require long-term management.1
Inflammatory Bowel Disease
IFN-γ, interferon γ; IL, interleukin; Th, T helper; TNF, tumor necrosis factor.
de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13-27. Salas A et al. Nat Rev Gastroenterol Hepatol. 2020;17:323-337.
IBD affects about 0.5% of the general population, but CD and UC have been reported to be 2-4× and 1.6-1.9× as frequent in patients with PsO, respectively.4-7 This known association appears to be rooted in a common dysregulation of the immune response in genetically susceptible individuals; among others, variants in several genes encoding for proinflammatory cytokine signals (eg, interleukin [IL]-12 or the IL-23 receptor) are correlated with both PsO and IBD.1,2,5–9 Notably, IBD is characterized by increased levels of several inflammatory cytokines, including IL-2 and interferon-gamma (IFN-γ) in CD, IL-5 in UC, and IL-17, IL-10, IL-1β, IL-6, and tumor necrosis factor (TNF) in both conditions.10,11 IL-17, IL-6, TNF-α, and IFN-γ are some of the key cytokines also involved in PsO pathogenesis.1,12,13 In the skin epithelium, IL-17 overexpression can trigger an inflammatory cycle, resulting in the formation of psoriatic plaques,13,14 whereas in the lamina propria of the gut, IL-17 supports neutrophil recruitment to promote inflammation and IL-22 mediated epithelial proliferation.10 This immune activation, acting alongside the release of further proinflammatory cytokines secreted by T-helper 1 cells, such as IL-6, TNF, and IFN-γ, inflames the epithelial cells that line the gut and ultimately damages them.10,15 This damage leads to barrier dysfunction, which allows the translocation of microbes into the bowel wall, attracting immune cells and amplifying inflammation.16,17
Inflammatory Bowel Disease
IFN-γ, interferon γ; IL, interleukin; Th, T helper; TNF, tumor necrosis factor.
de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13-27. Salas A et al. Nat Rev Gastroenterol Hepatol. 2020;17:323-337.
Because of the complex interplay between PsO and IBD, it is important for patients to be informed of their increased risk of developing this condition.4 Monitoring signs and symptoms of digestive tract disease in patients with PsO is especially important, as it would allow dermatologists to promptly refer patients in need for further evaluation and specialist care.4
References
- Fu Y et al. JAMA Dermatol. 2018;154:1417–1423.
- Yao D et al. Inflamm Bowel Dis. 2019;25:1595–1602.
- Schmitt H et al. Semin Immunopathol. 2019;41:737–746.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073–1113.
- Augustin M et al. Acta Derm Venereol. 2010;90:147–151.
- Cohen AD et al. J Eur Acad Dermatol Venereol. 2009;23:561–565.
- Li WQ et al. Ann Rheum Dis. 2013;72:1200–1205.
- Cho JH. Nat Rev Immunol. 2008;8:458–466.
- Cottone M et al. Dig Dis. 2019;37:451–457.
- de Souza HSP, Fiocchi C. Nat Rev Gastroenterol Hepatol. 2016;13:13–27.
- Fujino S et al. Gut. 2003;52:65–70.
- Kurtovic NO et al. Med Arch. 2018;72:410–413.
- Alwan W, Nestle FO. Clin Exp Rheumatol. 2015;33(suppl 93):S2–S6.
- Mahil SK et al. Semin Immunopathol. 2016;38:11–27.
- Salas A et al. Nat Rev Gastroenterol Hepatic. 2020;17:323–337.
- Neurath MF. Nat Rev Immunol. 2014;14:329–342.
- Marafini I et al. Expert Opin Biol Ther. 2019;19:1207–1217.