
This site is intended for US Healthcare Professionals only.
more than a skin disease
Metabolic Syndrome
Metabolic syndrome (MetS) is a collection of interrelated metabolic disorders, including obesity, hypertension, dyslipidemia, and insulin resistance, which can all contribute to the development of type 2 diabetes.1 This combination of disorders confers considerable disease burden, increases the risk of mortality, and significantly elevates the risk of developing subsequent cardiovascular (CV) disease, as well as stroke, fatty liver disease, and certain types of malignancy.1–3
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Metabolic Syndrome
MetS affects about 15%–25% of the general population, but its incidence is almost double (20%–50%) in patients with psoriasis (PsO) and is higher in women than in men.1,2,4,5 The risk of developing MetS is known to increase with PsO severity.1-5 The individual components of MetS are also significantly higher in patients with PsO vs controls; obesity is reported in 38% of patients with PsO vs 31% of healthy controls, elevated triglycerides are reported in 36% vs 28%, hypertension is reported in 31% vs 28%, and elevated glucose levels are reported in 22% vs 16%.2 Furthermore, those with severe and mild PsO have a 46% and 11% increased risk (respectively) of developing type 2 diabetes compared with those without PsO.6 Gout and hyperuricemia, which are tied to MetS and positively associated with CV risk, have also been reported to be associated with PsO.7 Assessment using the Framingham risk score found significantly higher risk for major cardiovascular events in patients with PsO.8 As a result of these serious connections to CV health, the American College of Cardiology/American Heart Association guidelines have been updated to include PsO as a risk factor for CV disease.9
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Metabolic Syndrome
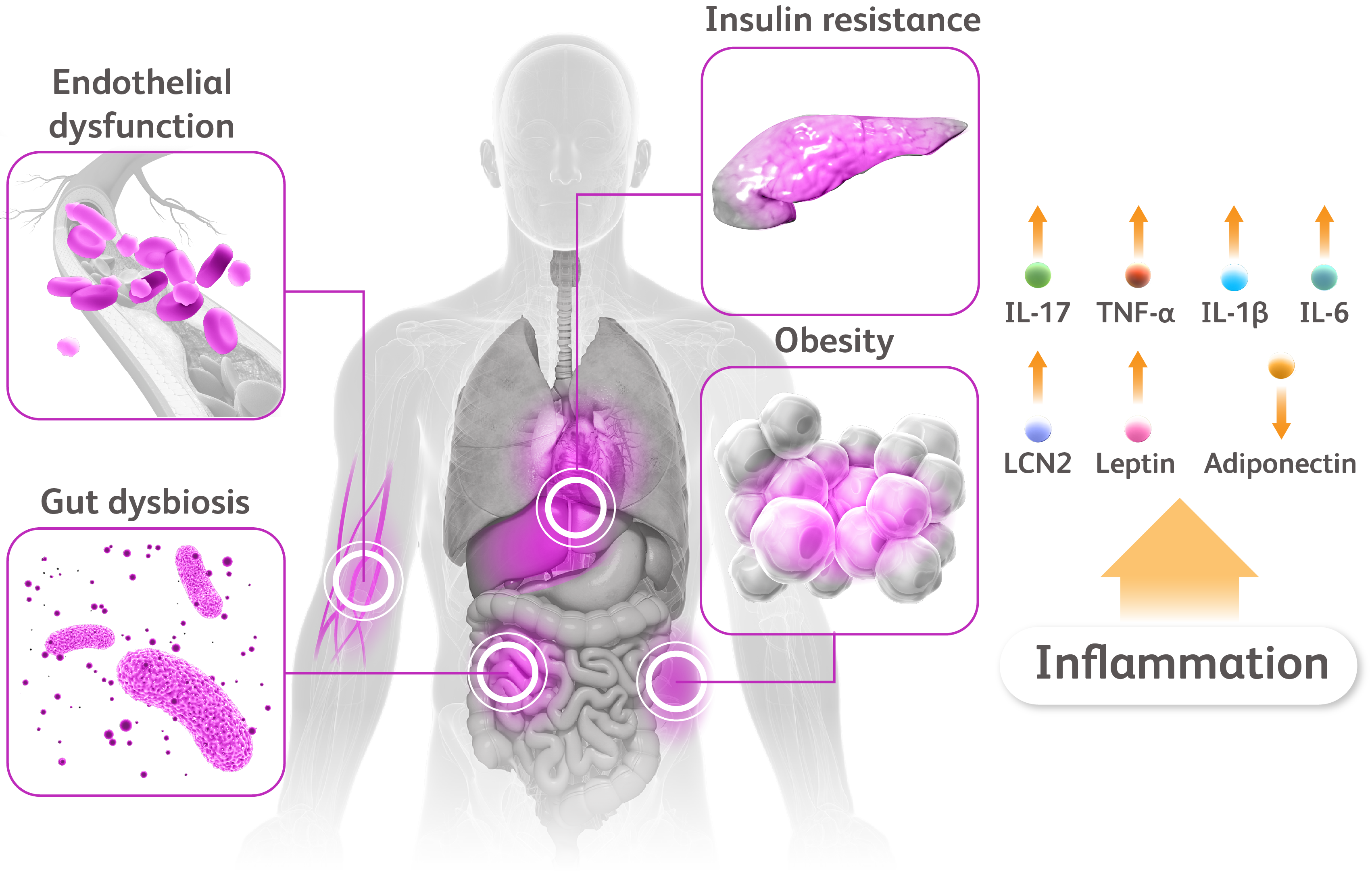
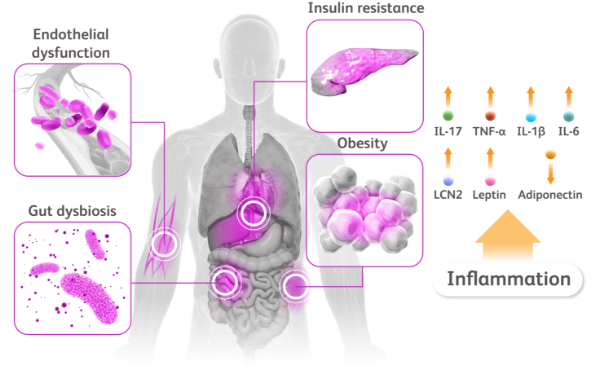
Although the pathologic mechanisms underlying the association between MetS and PsO are still unclear, several inflammatory cytokines seem to be involved in a shared etiology.1,10 In particular, interleukin (IL)-17 is emerging as a possible mediator between MetS and PsO, given its crucial role in the development and maintenance not only of psoriatic inflammation, but also of insulin resistance and type 2 diabetes.10 IL-17 also affects the levels of leptin, a critical hormonal regulator of metabolism whose serum level concentrations not only are elevated in both patients with obesity and patients with PsO, but also positively correlate with PsO severity.10–12 IL-17 also directly correlates with atherosclerotic plaque formation, and elevated levels of IL-17 in plasma are reported in unstable angina or acute myocardial infarction.13–15 Additionally, several other adipocytokines, including adiponectin, tumor necrosis factor alpha, IL-1β, IL-6, and lipocalin 2, may mediate the inflammatory pathways in PsO and MetS by modulating the inflammatory response that underlies both conditions.1,10–12,16,17
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Metabolic Syndrome
Other potential pathogenic mechanisms include the increased production of reactive oxygen species, a hallmark of oxidative stress-driven inflammation, and dysregulation of the gut microbiota, which is altered in both patients with PsO and in those suffering from MetS.11
Dermatologists could play a pivotal role in managing this set of comorbidities via early identification and prompt referral for assessment and treatment of the individual components of MetS.1,2 According to the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that patients with PsO should be informed about the risk for MetS and evaluated appropriately for CV and metabolic parameters.1,2
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Metabolic syndrome (MetS) is a collection of interrelated metabolic disorders, including obesity, hypertension, dyslipidemia, and insulin resistance, which can all contribute to the development of type 2 diabetes.1 This combination of disorders confers considerable disease burden, increases the risk of mortality, and significantly elevates the risk of developing subsequent cardiovascular (CV) disease, as well as stroke, fatty liver disease, and certain types of malignancy.1–3
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
MetS affects about 15%–25% of the general population, but its incidence is almost double (20%–50%) in patients with psoriasis (PsO) and is higher in women than in men.1,2,4,5 The risk of developing MetS is known to increase with PsO severity.1-5 The individual components of MetS are also significantly higher in patients with PsO vs controls; obesity is reported in 38% of patients with PsO vs 31% of healthy controls, elevated triglycerides are reported in 36% vs 28%, hypertension is reported in 31% vs 28%, and elevated glucose levels are reported in 22% vs 16%.2 Furthermore, those with severe and mild PsO have a 46% and 11% increased risk (respectively) of developing type 2 diabetes compared with those without PsO.6 Gout and hyperuricemia, which are tied to MetS and positively associated with CV risk, have also been reported to be associated with PsO.7 Assessment using the Framingham risk score found significantly higher risk for major cardiovascular events in patients with PsO.8 As a result of these serious connections to CV health, the American College of Cardiology/American Heart Association guidelines have been updated to include PsO as a risk factor for CV disease.9
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Although the pathologic mechanisms underlying the association between MetS and PsO are still unclear, several inflammatory cytokines seem to be involved in a shared etiology.1,10 In particular, interleukin (IL)-17 is emerging as a possible mediator between MetS and PsO, given its crucial role in the development and maintenance not only of psoriatic inflammation, but also of insulin resistance and type 2 diabetes.10 IL-17 also affects the levels of leptin, a critical hormonal regulator of metabolism whose serum level concentrations not only are elevated in both patients with obesity and patients with PsO, but also positively correlate with PsO severity.10–12 IL-17 also directly correlates with atherosclerotic plaque formation, and elevated levels of IL-17 in plasma are reported in unstable angina or acute myocardial infarction.13–15 Additionally, several other adipocytokines, including adiponectin, tumor necrosis factor alpha, IL-1β, IL-6, and lipocalin 2, may mediate the inflammatory pathways in PsO and MetS by modulating the inflammatory response that underlies both conditions.1,10–12,16,17
Metabolic Syndrome
IL, interleukin; LCN2, lipocalin 2; TNF, tumor necrosis factor.
Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386-1394. Gisondi P et al. Clin Dermatol. 2018;36:21-28. Hao Y et al. Front Immunol. 2021;12:711060. Karbach S et al. Arterioscler Thromb Vasc Biol. 2014;34:2658-68. Kong Y et al. Lipids Health Dis. 2019;18:171. Olejniczak-Staruch I et al. Int. J. Mol. Sci. 2021;22(3998):1-19. Wang D et al. Disease Markers. 2019;7361826:1-19. Wang Y et al. Clin Chem. 2007;53(1):34-41.
Other potential pathogenic mechanisms include the increased production of reactive oxygen species, a hallmark of oxidative stress-driven inflammation, and dysregulation of the gut microbiota, which is altered in both patients with PsO and in those suffering from MetS.11
Dermatologists could play a pivotal role in managing this set of comorbidities via early identification and prompt referral for assessment and treatment of the individual components of MetS.1,2 According to the AAD-NPF Guidelines of Care for the Management and Treatment of Psoriasis with Awareness and Attention to Comorbidities, it is recommended that patients with PsO should be informed about the risk for MetS and evaluated appropriately for CV and metabolic parameters.1,2
References
- Gisondi P et al. Clin Dermatol. 2018;36:21–28.
- Elmets CA et al. J Am Acad Dermatol. 2019;80:1073–1113.
- Armstrong AW et al. J Am Acad Dermatol. 2013;68:654–662.
- Armstrong AW et al. Nutr Diabetes. 2012;2:e54.
- Armstrong AW et al. JAMA Dermatol. 2013;149:84–91.
- Azfar RS et al. Arch Dermatol. 2012;148:995–1000.
- Merola JF et al. Ann Rheum Dis. 2015;74:1495–1500.
- Gisondi P et al. Am J Cardiol. 2010;106:1754–1757.
- Arnett DK et al. Circulation. 2019;140:e596–e646.
- Hao Y et al. Front Immunol. 2021;12:711060.
- Kong Y et al. Lipids Health Dis. 2019;18:171.
- Coimbra S et al. J Eur Acad Dermatol Venereol. 2010;24:1386–1394.
- Lockshin B et al. J Am Acad Dermatol. 2018;79:345–352.
- Perez-Chada LM, Merola JF. Clin Immunol. 2020;214:108397.
- Wu JJ et al. J Eur Acad Dermatol Venereol. 2022. doi: 10.1111/jdv.18044.
- Wang Y et al. Clin Chem. 2007;53(1):34–41.
- Wang D et al. Disease Markers. 2019;7361826:1–19.